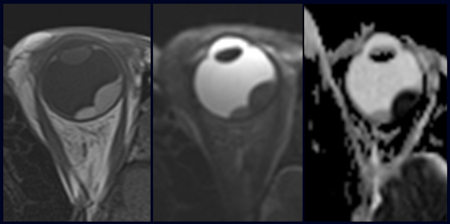
MUSHROOM CLOUD APPEARANCE ON CT/MRI
a.over 90%
b.over 70%
c.over60%
d.over50%
Q2.’Tram track’ sign on axial image and ‘doughnut sign’ on coronal image of orbit is seen in
a.optic nerve meningioma
b.optic nerve glioma
c.retinoblastoma
d.uveal melanoma
Q3..All are true regarding uveal melanoma except
a.most common intra-ocular malignancy in adults
b.hypodense on CT
c.hyperintense on T1W
d.hypointense on T2W
Q4..Intra-ocular mass giving appearance of ‘Mushroom cloud’ on CT/MRI is
a.retinoblastoma
b.optic nerve glioma
c.meningioma
d.uveal melanoma
ANS: 1---a
2---a
3---b
4---d
ROLE OF CT AND MRI IN ORBIT
- CT is useful because of the inherent natural contrast provided by the presence of structures with widely different attenuation coefficients (fat, bone, fluid, muscle, adjacent air) within a confined space.
- CT is preferred over MRI for detecting small calcified optic nerve meningiomas and in a child with suspected retinoblastoma, where detection of calcification is paramount.
- Overall, however, MRI is gaining more acceptance because of its greater sensitivity in characterizing diseases of the orbit (especially with use of fat-suppressed T1-weighted imaging, combined head and surface coils and faster data acquisition), and the far greater ability and versatility of MRI in detecting concomitant intracranial (especially intra-axial) abnormalities.
RETINOBLASTOMA
- Retinoblastoma is the most common tumour of the globe in children. It occurs in children less than 3 years of age presenting with leukokoria.
- 75 per cent are unilateral unifocal and 25 per cent are bilateral or unilateral multifocal.
- When it is found bilaterally and in conjunction with a pineoblastoma, it is labelled ‘trilateral retinoblastoma’
- 10–40 per cent are familial (autosomal dominant, with the oncogene present on chromosome 13), and these tumours tend to be bilateral and associated with other nonocular tumours.
- Retinoblastoma is highly malignant and may spread haematogenously, via lymphatics, or may spread along the optic nerve to the intracranial compartment to give drop metastases in the subarachnoid space.
IMAGING

- Imaging is crucial for timely management and survival of patients with retinoblastoma.
- CT is the preferred method to image the child with leukokoria because it is sensitive to calcification in retinoblastoma.
- CT demonstrates clumped or punctate calcification (in 95 per cent of cases) in the posterior part of the globe extending into the vitreous, with minimal enhancement.
- If CT shows calcification in an intra-ocular mass in a child less than 3 years of age, it should be considered a retinoblastoma until proven otherwise.
- Absence of calcification means this diagnosis is unlikely, since it is rare in other causes of leukokoria.
- On MRI, retinoblastomas are hyperintense on T1 and hypointense on T2, possibly due to calcification, or some other paramagnetic entity, or tumour protein.
- MRI is better for detection of tumour extension both along the optic nerve and intracranially.
MELANOMA
- Uveal melanoma is the most common primary intra-ocular malignancy in adults.
- The great majority are located unilaterally in the choroid. It can metastasize to the liver and lung.
- Diagnosis is usually performed on ophthalmoscopy and ultrasound (US).
- CT and MRI are not considered in the routine workup of this disease except when it is not possible to perform adequate ophthalmoscopy, e.g. in the presence of an opaque vitreous or when there are large subendothelial effusion(s).
- CT and MRI demonstrate a uveal melanoma as a soft tissue mass centred on the outer layers of the globe This mass bulges inward into the vitreous and may be small and flat or crescentic, or large and sharply demarcated with a ‘mushroom cloud’ appearance.
- On CT it is hyperdense and enhances after contrast medium administration.
- On MRI it is hyperintense on T1 and hypointense on T2 in melanotic melanomas due to the presence of paramagnetic melanin with/without haemorrhage.
- Amelanotic melanomas are hypointense on T1 and hyperintense on T2, as are other tumours. Both types of melanomas enhance on MRI.
- MRI is better than CT for adequate differential diagnosis with choroidal haemangiomas and choroidal detachments, and for better depiction of episcleral invasion
OPTIC NERVE MENINGIOMA

- Optic nerve meningiomas occur in middle-aged women, and more rarely in children with neurofibromatosis type 2.
- They are the second commonest primary tumours of the optic nerve after gliomas
- Hyperostosis in a remodelled widened optic canal may be present.
- Optic nerve meningiomas result usually in tubular thickening of the optic nerve/sheath complex rather than fusiform or excrescent thickening. Along with this thickening, the optic nerve tends to be seen as separate from tumour.
- 0n CT the tumour is hyperdense on CT and aenhance strongly producing a ‘tram track’ sign on axial images and a ‘doughnut sign’ on coronal images.
- Calcification (psammoma bodies) is common (20–50 per cent of cases). CT may be necessary to detect the linear calcification of early lesions.
- On MRI, these lesions are hypointense on T1 and hyperintense on T2. They again enhance strongly, especially appreciated with fat suppression . Early meningiomas are thus rendered more conspicuous on T1 fat-suppressed post-contrast images.
- Overall, MRI is better for orbital apex and intracanalicular lesions because surrounding bone makes this area difficult to outline accurately on CT.
OPTIC NERVE GLIOMA

- Optic nerve gliomas are childhood slow-growing low-grade pilocytic astrocytomas, with 75 per cent of cases occurring at less than 10 years of age.
- Bilateral tumours are virtually pathognomonic of neurofibromatosis. Optic nerve gliomas constitute 80 per cent of all primary optic nerve tumours.
- Optic nerve glioma results in tortuous thickening of the optic nerve/sheath complex that is most commonly tubular, but may also be fusiform or excrescent.
- Unlike optic nerve meningiomas, gliomas cannot be separated from the optic nerve itself
- Only half these lesions enhance, and they may contain cysts.
- Calcification is rare except post radiotherapy.
- MRI is necessary to detect involvement of the rest of the optic pathway because only 25 per cent of optic pathway gliomas are confined to the optic nerves.
- However, an optic nerve glioma does not itself tend to spread from the optic nerve to the intracranial compartment.
- MRI shows these lesions as isointense on T1 and hyperintense on T2.
REF:
No comments:
Post a Comment