New research from Mayo Clinic demonstrates that using molecular breast imaging (MBI) as an adjunct to mammography results in an almost four-fold increase in invasive cancer detection in women with dense breast tissue. These findings, along with results of earlier studies, have spurred the Rochester, Minn., clinic to make supplemental imaging with MBI its standard of care for women with dense breasts.
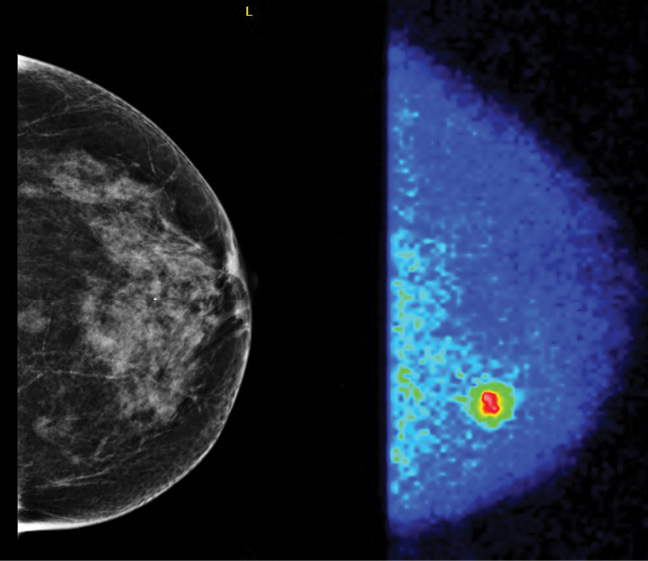
MBI utilizes a small gamma camera to acquire images of the breast after injection of the radiotracer sestamibi.
"Breast tumors very avidly take up sestamibi," said Dr. O'Connor, who collaborated on the research with radiologists, surgeons and physicians at the Breast Diagnostic Clinic at Mayo Clinic in Minnesota. "With this technique, we're not looking at the architecture of the lesion, but rather its metabolic activity."
Breast imaging expert Wendie Berg, M.D., Ph.D., professor of radiology at Magee-Womens Hospital of the University of Pittsburgh School of Medicine, said the findings show a potential role for MBI in screening the approximately 40 percent of women over age 40 who have dense breasts.


